Conclusion
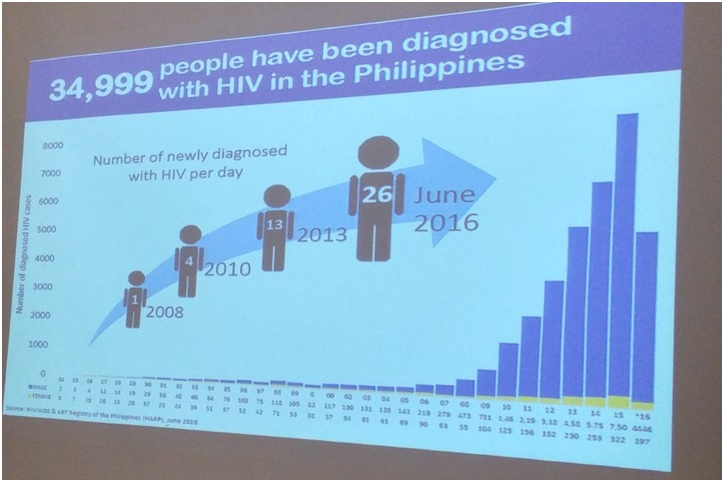
AS the Philippines emerged as one of the countries with accelerating rates of new cases of persons with human immunodeficiency virus (HIV), staging more efficient information dissemination on HIV is gnarly for health authorities.
Assistant Health Secretary Enrique A. Tayag said that, with the P400-million funding for HIV/AIDS, the Department of Health (DOH) would like to focus on prevention “rather than treatment”.
Tayag said persons living with HIV acquired immunodeficiency syndrome (AIDS) who are enrolled in the Philippine Health Insurance Corp. (PhilHealth) can receive specific benefits and assistance.
Tayag was referring to the PhilHealth Outpatient HIV/AIDS Treatment (OHAT) package that covers antiretroviral treatment (ART) and laboratory exams based on specific treatment guideline. These guidelines cover CD4 cell determination, viral load test, drug-toxicity test and professional fees of providers.
The package covers up to P30,000 worth of necessary medical expenses per member-patient per year.
PhilHealth will be paying a maximum of P30,000 ($599.41, at current exchange rates) per year without cap on how many times the patient will go to treatment hubs and how many medicines or tests the patient will avail himself or herself, as long as it falls within the given amount. The OHAT package goes in accordance with the guidelines set by the DOH. According to Tayag, who is also the DOH spokesman, the department is giving P15,000 ($299.71) per person per year for first line drug and P80,000 ($1,598.44) per person per year for second line drugs.
Testing
HEALTH Secretary Paulyn Jean B. Rosell-Ubial said the DOH is continuously
offering free and confidential HIV testing in social-hygiene clinicsrun by local government units and in 22 HIV
Treatment Hubs nationwide.
Ubial added that the DO wH is also providing free condoms. Kits are not available to the public as counseling is required before and after testing, she explained.
The DOH chief said treatment options are available to those who test positive for HIV. ARTs are applied to individuals who need to lower the viral load of patients and to improve their immune response.
The DOH is seriously considering a recently-announced World Health Organization (WHO) recommendation on self-testing to improve HIV-testing rates and prevent treatment delays, according to Ubial. The Philippine National AIDS Council of the DOH is committed to end the spread of HIV and improving the lives of all who live with it, she added. She said the Sixth AIDS Medium Term Plan (AMTP), which “is the blueprint of our national response” on HIV and AIDS have determined the targets for 2022.
Ubial said the government is optimistic on reversing HIV trends in the next six years but “only if an ‘All of Society’ and ‘HIV in All of Policies’ approaches are sought with renewed vigor and determination.”
“The ‘All for Health towards Health for All’ line resonates for stopping HIV,” she said adding, that the global call for “Hands Up for HIV” prevention “has just turned a new leaf in the Philippines.”
Non-governmental
OUTSIDE of the government are initiatives by private groups and advocates addressing the HIV/AIDS pandemic.
One is the Philippines’s business of Johnson & Johnson Inc. Weeks after losing a lawsuit in the US on its baby-powder product, Johnson & Johnson Philippines launched late last month a campaign the company calls “a comprehensive HIV disease-management program.”
Developed by the Janssen Pharmaceutical Cos. of Johnson & Johnson, the program tapped non-governmental organization (NGO) Sustained Health Initiatives of the Philippines Inc. (Ship). Ship has been running a specialist HIV care center with the Philippines General Hospital in Manila. According to documents it provided, the organization “offers high-quality, affordable HIV and primary care directly to the communities that need it most.”
According to Janssen, the program also targets to improve the understanding of the attitudes people hold toward HIV and the factors that affect patient adherence to their medicines, as well as how well treatments work and the availability of ongoing care. Working together, Johnson & Johnson (Philippines) Inc. and Ship “will undertake essential research into current awareness and attitudes toward HIV in the Philippines to generate the necessary evidence to guide education and treatment practices.
“Our goal is to improve the lives of those affected by HIV and significantly reduce the incidence of the disease,” Janssen’s Disease Management Programs leader Dr. Randeep Gill said during the launch of the program called “Connect for Life”. “Health-care solutions and appropriate care planning must be centered around patients’ needs.”
According to Gill, the program will use an evidence-based approach in designing and developing “integrated healthcare solutions focusing on patients’ and health-care worker’s needs and support the implementation of structured interventions to turn the tide on an increasing epidemic.”
Leverage
THE Philippines is one of seven countries in the world where HIV infection rates are increasing. It had the highest proportional increase of infections among the 15- to 24-year-old age range from 2005 to 2015, documents provided by Janssen said.
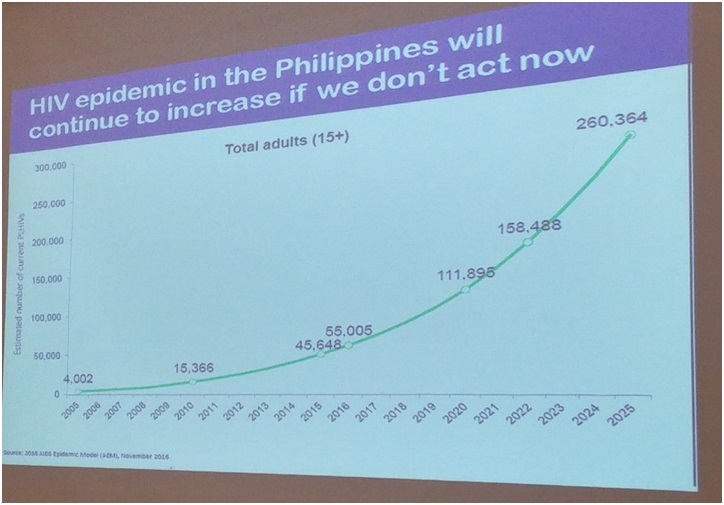
The number of people living with HIV is anticipated to increase substantially by 2022. The quality of HIV care in the country is varied, with time from diagnosis to treatment and level of stigma differing greatly between regions.
The diverse geography of the Philippines often limits access to health-care services and improved interconnectivity between health providers could reduce variations in quality of care across the islands, according to documents provided by Janssen.
The company said the program offers treating physicians a clinical information system to further engage with their patients and offers patients the means to stay connected across remote locations.
Johnson & Johnson Philippines Inc. Managing Director Jeffrey Go said “the collaboration forms part of an ongoing effort to leverage the strengths of Johnson & Johnson and bring forth innovative programs to improve health outcomes.”